
In Short: What is Pelvic Organ Prolapse?
Pelvic Organ Prolapse (POP) occurs when one or more of the pelvic organs (the bladder, uterus, or rectum) drop from their normal position and bulge into the vagina. This happens due to a weakening or damage of the pelvic floor muscles and connective tissues that support these organs. It’s not life-threatening, but it can significantly affect your quality of life, physical comfort, and confidence. Many women with prolapse experience associated symptoms like urinary incontinence, difficulty with bowel movements, or pain during sex.
Why This Matters
I’ll never forget the first time a client described her prolapse to me. She said it felt like “something falling out” of her body. She was terrified to exercise, afraid to lift her toddler, and had stopped having sex with her partner because she was so self-conscious about the bulge. She told me she felt broken, like her body had betrayed her.
That conversation stayed with me because I hear versions of it all the time. Different words, same underlying fear and shame.
There’s the runner who gave up her morning jogs because the heaviness got worse with every stride. The mum who stopped playing on the floor with her kids because getting up felt like everything was going to fall out. The woman who planned her entire day around when she felt “best”, usually first thing in the morning before gravity had done its work.
Pelvic organ prolapse isn’t just a physical issue. Yes, there’s the sensation of heaviness, the bulge you can feel or see, the difficulty emptying your bladder or bowels. But what really gets to women is how it makes them feel about their bodies.
The constant awareness. The monitoring. The fear that it’s getting worse. The worry that everyone can somehow tell. The loss of spontaneity because you need to plan around how your body feels.
Here’s what I need you to understand: prolapse doesn’t have to define your life.
Addressing prolapse is about restoring physical comfort, yes. But it’s also about regaining confidence and enabling you to live a full, active life without the constant worry and physical burden. It’s about feeling like yourself again.
With the right approach many women can see significant improvement in their symptoms. Some avoid surgery entirely. Others find that conservative treatment gives them the confidence and strength they need before considering surgical options.
I’ve seen women go from feeling terrified to move to running half-marathons. From avoiding intimacy to reconnecting with their partners. From planning their lives around their prolapse to barely thinking about it.
Yes, prolapse is common, about 50% of women who’ve had children experience some degree of it. But common doesn’t mean you have to accept it as your reality. Your body is capable of healing and adapting.
What is Pelvic Organ Prolapse?
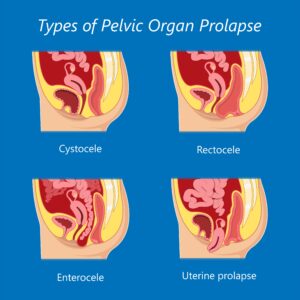
First Image (Normal Anatomy): The bladder, uterus, and rectum are in their correct positions, supported by the pelvic floor muscles that look like a taut hammock running from the pubic bone to the tailbone.
Subsequent Images: Illustrations showing a Cystocele (bladder bulging into the front vaginal wall), Rectocele (rectum bulging into the back vaginal wall), and Uterine Prolapse (uterus descending into the vaginal canal). Arrows indicate the direction of organ descent.
Understanding the Anatomy
To understand prolapse, you need to visualise the pelvic floor as a complex network of muscles, ligaments, and fascia that forms a supportive sling at the base of your pelvis. This intricate structure acts as a hammock, holding the pelvic organs, the bladder, uterus, and rectum, in their correct anatomical positions.
Think of it like a trampoline or a suspension bridge. The muscles provide the active support (they can contract and relax), while the ligaments and fascia provide the passive support (they hold things in place). When this support system is compromised, either the muscles weaken or the connective tissue stretches, and the organs can descend.
The pelvic floor is designed to withstand downward pressure from the abdomen. Every time you cough, sneeze, lift something, or even just stand up, there’s pressure pushing down on these organs. In a healthy system, the pelvic floor pushes back, keeping everything in place.
But when this pressure is chronic or excessive, or when the pelvic floor tissues are weakened (from childbirth, hormonal changes, chronic straining), the organs can be pushed downwards into the vaginal space.
Types of Prolapse
The specific type of prolapse depends on which organ descends:
Cystocele (Bladder Prolapse): The bladder bulges into the front wall of the vagina. This is the most common type. You might notice difficulty emptying your bladder completely, frequent urination, or a bulge you can feel at the front of your vaginal opening.
Rectocele (Rectum Prolapse): The rectum bulges into the back wall of the vagina. This often causes difficulty with bowel movements, you might need to apply pressure to the perineum or vagina to help empty your bowels (what we call “splinting”), or feel like you can’t completely empty.
Uterine Prolapse: The uterus descends into the vaginal canal. In severe cases, it can protrude outside the vaginal opening. You might feel a bulge, heaviness, or like something is “falling out.”
Enterocele (Small Bowel Prolapse): The small intestine pushes into the upper part of the vagina. This is less common but can cause a feeling of pressure high in the vagina.
Vaginal Vault Prolapse: After a hysterectomy, the top of the vagina itself can drop down. This happens because the uterus, which provided some structural support, has been removed.
Grading Prolapse
Prolapse is graded on a scale, typically from Stage 1 (mild) to Stage 4 (severe):
- Stage 1: The organ has dropped slightly but is still well within the vagina
- Stage 2: The organ has dropped to the vaginal opening
- Stage 3: The organ protrudes outside the vaginal opening
- Stage 4: Complete prolapse – the organ is fully outside the body
Here’s something really important: the grade doesn’t always correlate with symptoms. I’ve worked with women who have Stage 2 prolapse and are incredibly bothered by it, and others with Stage 2 who barely notice. Treatment is based on how much it affects your quality of life, not just the grade.
Causes and Risk Factors
Pelvic organ prolapse is multifactorial; it arises from a combination of factors that weaken the pelvic floor support structures over time. Understanding these causes is key to both prevention and effective management.
1. Pregnancy and Childbirth
This is the most significant risk factor for prolapse. The prolonged strain of pregnancy, coupled with hormonal changes that soften connective tissues, can stretch and weaken the pelvic floor. Your body releases relaxin, which makes tissues more elastic to allow for birth, but this also means everything stretches more easily.
Vaginal delivery, especially with prolonged pushing, instrumental delivery (forceps or vacuum), large babies, or episiotomy, can directly damage muscles and nerves. According to the NHS, pregnancy and childbirth are the biggest risk factors for developing prolapse, with the risk increasing with each vaginal birth.
Even caesarean sections don’t entirely eliminate risk. The weight of pregnancy itself, those nine months of carrying a baby, contributes to pelvic floor strain and can weaken the fascial support system.
2. Chronic Increased Intra-Abdominal Pressure
Repeated or sustained increases in pressure within the abdominal cavity can push down on the pelvic floor, gradually weakening its supportive structures. Common sources include:
Chronic Coughing: Often due to smoking, asthma, or chronic bronchitis. Every cough creates a spike of downward pressure.
Chronic Constipation and Straining: Persistent bearing down during bowel movements is highly detrimental. If you’re straining daily for years, you’re essentially training your pelvic floor to weaken.
Heavy Lifting: Occupational or recreational heavy lifting without proper core engagement and breathing technique.
High-Impact Exercise: Activities like jumping or running, if the pelvic floor isn’t adequately supported, can contribute to prolapse over time.
3. Hormonal Changes (Menopause)
Oestrogen plays a vital role in maintaining the strength, elasticity, and health of connective tissues throughout the body, including the pelvic floor. During perimenopause and menopause, the decline in oestrogen levels can lead to thinning and weakening of these tissues, making them less able to support the pelvic organs. Research published in the American Journal of Obstetrics and Gynecology shows that postmenopausal women have significantly higher rates of prolapse due to these hormonal changes.
This is why some women who’ve never had symptoms suddenly notice prolapse in their 50s or 60s. The tissues that were holding everything in place have thinned and weakened.
4. Genetics and Connective Tissue Disorders
Some women are genetically predisposed to weaker connective tissues, making them more susceptible to prolapse. If your mother or sisters have prolapse, you’re at higher risk. Conditions like Ehlers-Danlos syndrome, which affect collagen production, can also significantly increase risk.
5. Obesity
Excess body weight, particularly abdominal obesity, places a constant downward load on the pelvic floor, increasing intra-abdominal pressure and contributing to the weakening of supportive tissues. Studies show that maintaining a healthy weight is one of the most important modifiable risk factors for preventing prolapse.
6. Prior Pelvic Surgery
Hysterectomy (removal of the uterus) can sometimes alter the support structures of the vagina, potentially increasing the risk of vaginal vault prolapse later in life. The uterus provides some structural support, and when it’s removed, the top of the vagina can drop down.
Symptoms and Diagnosis
The symptoms of prolapse can vary wildly depending on which organ is affected and how severe it is. I’ve worked with women who have mild prolapse and feel absolutely fine, they only discovered it during a routine exam. And I’ve worked with others who are really struggling, even though technically their prolapse isn’t that advanced.
Common Symptoms
That Dragging, Heavy Feeling: This is what most women describe first. A feeling of fullness, like something’s falling out of your vagina. It’s usually worse by the end of the day or after you’ve been on your feet for ages. Many women tell me it feels like they’re “sitting on a ball” or that something’s going to drop out. It’s unsettling, to say the least.
A Bulge You Can Feel or See: In more advanced cases, you might actually feel or see a bulge at your vaginal opening. Some women notice it in the shower or when they’re using the toilet. It can be really alarming the first time you discover it.
Bladder Issues:
If your bladder is prolapsing (cystocele), you might struggle to empty it completely. You might be running to the loo constantly or leaking when you cough or sneeze. Some women tell me they need to push the bulge back in to fully empty their bladder.
Bowel Problems:
If it’s your rectum (rectocele), bowel movements can become difficult. You might need to press on your perineum or the back wall of your vagina to help things along, what we call “splinting.” It’s not something anyone talks about, but it’s more common than you’d think. Or you might feel like you can never quite empty properly.
Sex Becomes Uncomfortable:
Pain during sex, reduced sensation, or just feeling self-conscious about the bulge, all of this affects intimacy. Some women lose sensation. Others find certain positions uncomfortable.
Lower Back Ache:
Your body’s trying to compensate for the lack of support in your pelvis, which creates tension and pain elsewhere. It’s all connected.
How It’s Diagnosed
Getting a diagnosis usually means seeing a women’s health physio, gynaecologist, or urogynaecologist. I know it can feel daunting, but honestly, these professionals see prolapse every single day. There’s nothing to be embarrassed about, they’ve seen it all.
They’ll Ask About Your History: Your symptoms, pregnancies, births, lifestyle. Be really honest about what you’re experiencing. The more they know, the better they can help. Don’t downplay things or feel like you’re making a fuss.
The Pelvic Exam: This is the important bit. You’ll usually be examined lying down and sometimes standing. They might ask you to cough or bear down so they can see how far things descend. They’re checking your pelvic floor strength too; can you squeeze? Can you hold it? Can you fully relax afterwards? It might feel awkward, but it’s so valuable. You’ll finally understand what’s actually happening inside your body.
Questionnaires: Sometimes they’ll give you forms to fill out about how your symptoms affect your daily life. This helps track your progress over time, which is really motivating when you start to see improvements.
Imaging: Not usually necessary, but sometimes they’ll use MRI or ultrasound if they need more detail, especially if surgery’s being considered.
Treatment Options
Right, so here’s where it gets interesting. Treatment for prolapse ranges from “let’s try some exercises and lifestyle changes” all the way to surgery. But here’s the thing, surgery should really be a last resort. For most women, conservative treatment works brilliantly.
1. Hypopressives (Low Pressure Fitness)
I’m obviously going to talk about Hypopressives for prolapse first because this is what transformed my own recovery and what I’ve seen work for hundreds of women. Hypopressives focus on reducing the pressure that’s pushing down on your pelvic floor and creating an upward lift of your organs. It’s literally working against gravity.
How It Actually Works: You use specific postures combined with a breath-hold (we call it an Apnea). This creates a vacuum effect inside your abdomen. That vacuum lifts your diaphragm and your pelvic organs upward, taking pressure off your pelvic floor. At the same time, it reflexively activates your deep core and pelvic floor muscles, without you having to consciously squeeze. It’s training your body to support itself automatically.
What I love about this approach is that it:
- Reduces that downward pressure that’s making everything worse
- Improves your pelvic floor tone without you having to think about it constantly
- Strengthens your entire core as one integrated system
The Research Bit: There’s a systematic review from 2024 in the American Journal of Surgery that compared pelvic floor exercises with Hypopressives for prolapse. Both worked well, but Hypopressives showed particular benefit for that sensation of heaviness and bulging, which is what really bothers women day-to-day.
I’ve personally found that doing a solid Hypopressives practice makes such a difference. Some women avoid practice on their heaviest symptom days, but if you feel up to it, even a short practice can help. It’s something to experiment with and see what works for you.
2. Pelvic Floor Muscle Training (Kegels)
Kegels are what most GPs recommend first. They involve consciously squeezing and lifting your pelvic floor to build strength. NICE guidelines recommend supervised pelvic floor training as first-line treatment.
But here’s the catch, they need to be done correctly. You should feel a lift and squeeze, not a bearing down or pushing out. So many women are doing them wrong, which is why working with a women’s health physio, at least initially, is so valuable.
3. Pilates and Yoga
When adapted properly for prolapse, postnatal Pilates and Yoga are invaluable. They improve your body awareness, your posture, your core strength, all without increasing that downward pressure.
Pilates focuses on deep core engagement and alignment. Modified Pilates can build strength without making your symptoms worse. The key is finding someone who understands prolapse and can adapt exercises appropriately.
Yoga can help release tension in your pelvic floor (which can actually be a factor in some prolapse cases) and improve mobility. The breathing work in yoga is brilliant for pressure management too. Inversions, like legs up the wall, can feel wonderful because they temporarily reverse gravity’s effects.
4. Pessaries
A pessary is a silicone device that sits inside your vagina and physically supports your prolapsed organs. It can be a game-changer for some women, and you can use it long-term if needed.
They come in different shapes, rings, cubes, Gellhorns, donuts. A healthcare professional fits you with the right one. Some women manage their own, taking them out and cleaning them regularly. Others have them managed by their GP or physio.
I have clients who use pessaries as a “bridge”, they wear them on high-activity days (when they’re exercising or on their feet loads) and take them out at other times. It gives them confidence to stay active while they’re building strength.
5. Lifestyle Changes
Weight: If you’re carrying extra weight, losing even 5-10% can make a noticeable difference. It’s not about how you look, it’s about reducing the constant load on your pelvic floor.
Constipation: This is massive. Straining on the toilet is one of the worst things for prolapse. High-fibre diet, plenty of water, and use a footstool (like a Squatty Potty) to get your knees higher than your hips. This changes the angle and makes everything easier.
Lifting: Learn proper technique – exhale as you lift, engage your core, keep things close to your body. If something feels too heavy, it probably is. Ask for help.
Chronic Cough: If you’ve got a persistent cough from smoking, asthma, or allergies, get it sorted. That constant pressure is working against all your rehab efforts.
6. Surgery
For severe prolapse, or when you’ve genuinely tried everything else and it’s not working, surgery might be an option. The goal is to put everything back where it should be and reinforce the support.
There are different surgical techniques depending on your situation, your age, whether you want more children, your sex life, the type of prolapse. It’s usually considered after you’ve exhausted conservative options.
Here’s the thing though, surgery doesn’t guarantee it won’t happen again. If you don’t address the underlying pressure issues, prolapse can recur. That’s why pelvic floor work is important both before and after surgery.
Recovery Timeline
Recovery from prolapse is different for everyone. It depends on what type you have, how severe it is, how consistent you are with treatment, and your overall health. The main thing is to be patient with yourself.
First 3 Months: This is about managing symptoms and building awareness. With consistent Hypopressives and pelvic floor work, most women notice less heaviness and bulging. You’re improving your pelvic floor tone and retraining how your body manages pressure. You might notice the bulge isn’t as prominent, or the heaviness isn’t as bad by evening.
3-6 Months: This is when things really start to shift. Your muscles are getting stronger and more coordinated. You’ll notice more sustained improvement and you can do more without symptoms flaring up. This is when women start feeling genuinely hopeful about getting back to normal life.
6+ Months: Prolapse is often something you manage long-term rather than “cure.” But many women manage it conservatively for years, decades even, without needing surgery. It’s about integrating the preventive strategies into your life and keeping up with your Hypopressives practice. It’s never too late to start. I’ve worked with women in their 60s and 70s who’ve made remarkable improvements.
When to See a Specialist
Conservative management works brilliantly for loads of women, but sometimes you need professional help. Don’t wait if you’re experiencing any of these.








